
Lung Cancer Choices© 6th Edition Menu
Sexuality and Lung Cancer
Jenna Kahn, MD and Loise W. Wairiri, MD
Introduction
Sexuality is defined as a central aspect of being human throughout life which encompasses sex, gender identities and roles, sexual orientation, eroticism, pleasure, intimacy, and reproduction (Figure 1). It is experienced and expressed in thoughts, fantasies, desires, beliefs, attitudes, values, behaviors, practices, roles, and relationships. While sexuality can include all these dimensions, not all of them are always experienced or expressed. Sexuality is influenced by the interaction of biological, psychological, social, economic, political, cultural, legal, historical, religious, and spiritual factors.1
Figure 1: Components of Sexuality
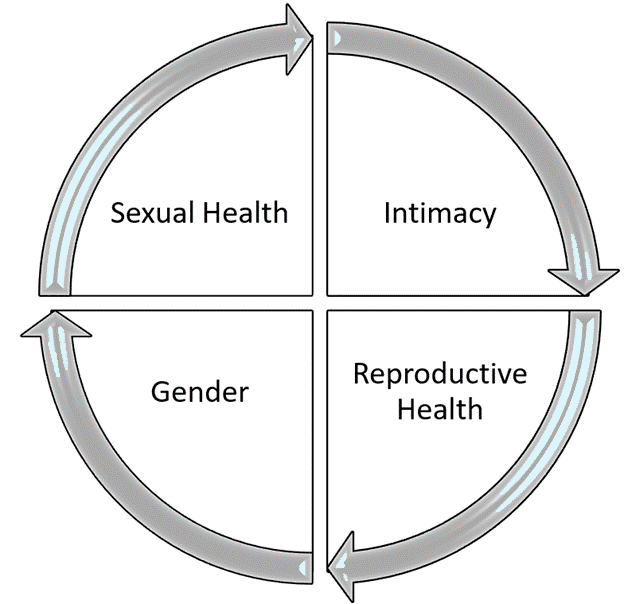
Sexuality-related concerns such as sexual health, intimacy, reproductive health, and gender are prevalent among cancer patients from diagnosis, during treatment, and can even extend years after primary management.2 In this chapter, we will discuss sexuality concerns, mechanisms, how they relate to cancer, and interventions.
Defining Sexual Health in Cancer Survivorship
Sexual health is an essential aspect of quality of life that requires a positive and respectful approach to sexuality and sexual relationships.3 Often, sexuality in cancer management suffers thus affecting the quality of life in these patients.
Reduced sexual function is a common distressful consequence of lung cancer diagnosis and treatment. The estimated prevalence of sexual dysfunction in cancer patients ranges from 40% to 100%, depending on the type of cancer, treatment modality, and methods of assessment.4 In lung cancer patients, the prevalence has not been well documented. However, studies show that sexual function progressively worsens over the lifetime of the patients.5 Lung cancer patients and their partners suffer significant physical and psychological distress because of a cancer diagnosis and management. Data suggests that substantial disruptions in psychological well-being impact patient’s sexual functioning, social well-being, and quality of life.6 In addition to the effects of cancer diagnosis and treatment, older age, and comorbidities such as diabetes, arthritis, and congestive heart failure worsen and increase concerns about sexuality.7
Lung cancer management has often minimized sexual health and focused on short-term quality of life improvement and palliative care. Conversations surrounding sexual health in cancer patients have been largely neglected.8 A study examing lung cancer treatment effects on sexuality reported that 51.7% of patients had self-reported sexual concerns. Of these patients, 24.7% had moderate to severe sexual concerns.9 Despite these numbers, cancer care providers and patients express that sexual health issues are poorly addressed or adequately treated during cancer management.10-12 Poor patient-provider communication is a significant barrier to sexual health management in oncology as patients may feel unsupported and uncomfortable discussing their sexuality concerns openly.13-14 Patient interactions with health care providers during cancer management and follow-up are great opportunities to discuss quality of life issues including sexuality and sexual health.  An interactive cancer management approach ensures the patient always feels supported during care.
An interactive cancer management approach ensures the patient always feels supported during care.
Intimacy in Cancer Patients
According to the American Psychological Association (APA), intimacy is defined as an interpersonal state of emotional closeness. It characterizes familiar, close, and usually affectionate or loving personal relationships that require parties to have detailed knowledge or deep understanding of each other.15 Intimate relationships are vital to human beings but often suffer when partners suffer from significant or chronic illnesses like cancer.
Cancer diagnosis and treatment are stressful and cause significant distress to the physical and psychological well-being of cancer patients and their partners. As a result, it significantly strains the intimate relationships between cancer patients and their partners. Fatigue, pain, body image concerns, self-esteem and worth, depression, and anxiety are reasons why intimacy in relationships can be affected.16
Patients and partners have unique experiences and valid concerns during cancer diagnosis and management. Communication, assessment, and evaluation by the cancer care team can help tailor interventions best suited to the patient and their partner. Briefly, some of the ways to manage intimacy issues and concerns include; patients and partners seeking professional help from their cancer care team, establishing open communication with each other, and making necessary adjustments to accommodate for physical and emotional symptoms such as fatigue, pain, shortness of breath, low energy or moods, validating each other’s feelings, and setting time when appropriate for closeness and reacquaintance with each other.16
Reproductive Health Concerns in Lung Cancer Patients
Cancer diagnosis and treatment are often a threat to fertility in reproductive-aged patients. Although statistically most patients with lung cancer are past childbearing age, a few patients are diagnosed with lung cancer during the reproductive age group.
Infertility is a failure to conceive after one year of intercourse without contraception and may be permanent or transient. Causes of compromised fertility vary and include; side effects of cancer treatment (chemotherapy, radiation therapy), age, psychological effects of the disease, and treatment.17
Depending on the patient, different methods to restore/preserve fertility exist and should be discussed by the primary care and cancer care team at diagnosis or before treatment starts such as chemotherapy and radiation therapy. There are evidence-based guidelines on fertility preservation options for men and women and guidance from oncologists and cancer care providers.
Mechanisms of Sexual Dysfunction in Cancer Patients
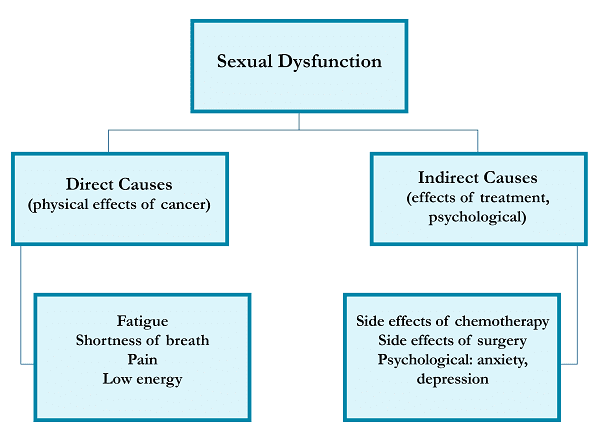
The patient’s ability for intimacy and sexuality can be affected by various factors that directly or indirectly stem from the disease. Symptoms of lung cancer independently contribute to decreased sexual function among patients and include pain, fatigue, and shortness of breath. The functional status of lung cancer patients correlates to sexual concerns in these patients.10 Factors contributing indirectly include psychological stressors and adverse effects of cancer treatment (surgery, chemotherapy, radiation therapy).18 A summary of the causes of sexual dysfunction is shown in Figure 2.
Figure 2: Causes of sexual dysfunction in cancer patients
Psychological distress
Depression and anxiety are prevalent among cancer patients with studies reporting rates of up to 43.4% in lung cancer patients.19 Anxiety and depression are associated with a decline in sexuality. As a result of the high rates of psychological distress in cancer patients, reduced sexuality is prevalent in this population.20
Anticancer therapies
Chemotherapy and surgery are significantly associated with decreased sexual function in lung cancer patients.
Surgery for lung cancer can decrease the sexual functioning of patients due to its invasive nature and increased physiological demands. Increased fear and anxiety post-operatively also contribute to decreased sexual functioning among patients undergoing surgery for lung cancer. Depression and anxiety are especially prevalent in patients with lung cancer post-operatively.21
Chemotherapy for lung cancer is associated with fatigue, psychosocial and physical symptoms, and increased distress, all of which can reduce sexual function in these patients.22
Management of Sexual Dysfunction in Cancer Patients
The first step towards managing the concerns in intimacy and sexuality is holding discussions on the same throughout treatment and follow-up. Issues with intimacy and sexuality are important medical conditions just as any other medical conditions that need to be addressed. Health care providers are not bothered or too busy to handle such issues and according to the American Society of Clinical Oncology (ASCO), they should initiate discussions on sexual health and dysfunction with the patients.4 We encourage patients to have a discussion openly with their health care provider at any time during cancer management. The choice to include the partner in the conversation should be made if the patient wishes. Sometimes patients may feel uncomfortable bringing up sexual concerns with the cancer care team and in that case, should bring them up to the primary care physicians. Below are some phrases that can be used to bring up discussions on sexuality.23
- “I’m curious about sexual health issues in patients with lung cancer. Could you speak more to this?”
- At the start of a new treatment, “How may my sexual health be affected by this new treatment?”
- “In my research, I have found that sexual health issues are common in patients with lung cancer, I would like to talk more about this.”
- “I want to discuss how my cancer may affect my sexual intimacy as my sexual drive and libido have decreased. Can we discuss how this relates to my cancer?
Management and Evaluation of Sexual Health
Pre-treatment counseling and routine assessment
It is critical to understand before and during cancer treatment that reduced sexual function is among the adverse effects encountered. This varies from patient to patient and the degree of dysfunction also varies throughout cancer management. Providers having baseline information on your pre-treatment/pre-diagnosis sexuality allows for easier follow-up and addressing any sexual concerns as soon as they arise. As discussed earlier, the causes of declining sexual function are varied and include; psychological stressors (anxiety, depression), physical stressors (fatigue, shortness of breath, pain), and psychosocial stressors (financial, familial, occupational, marital). They all affect individuals differently and addressing these causes with your health care provider is essential in management.18
Communication and involving the partner
Patients and their partners both undergo distressful phases that may cause intimacy concerns in the duration of cancer management. Communication with health care providers is important to establish goals and treatment outcomes for sexual function. Including partners in these discussions when the patients are willing and comfortable may offer better perspectives on expected course and outcomes during cancer management.24
Specific management
Information on managing sexual problems and concerns below has been sourced from the ASCO recommendations. Access to sexual health resources and referral information for the patient and partner is available from the health care providers (Figure 3).
Figure 3: Summary of the management of sexual dysfunction
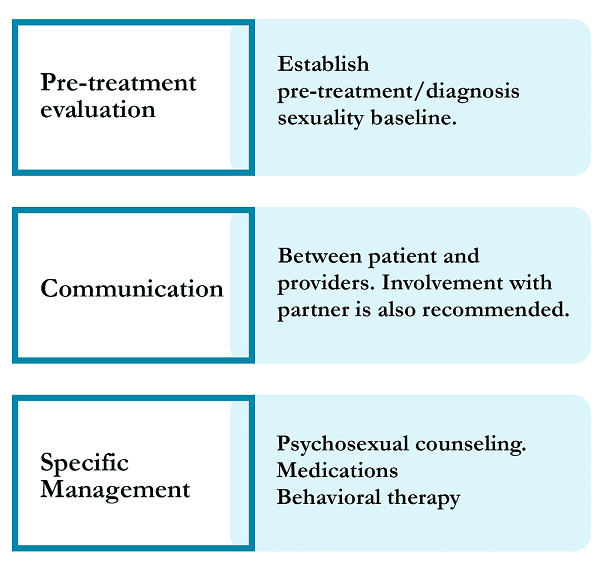
Psychosocial/psychosexual counseling should be offered to all cancer patients to improve sexual functioning. Current evidence does not support any one type of counseling over the other. Counseling is beneficial for cancer patients who are experiencing body image issues, patients looking to improve intimacy and sexuality issues, and also to enhance overall sexual functioning and satisfaction.4 Regular stimulation may also be helpful for patients experiencing sexual difficulties.
Specific medications can also be used to reduce symptoms and improve sexual function. These medications are tailored to men and women depending on their symptoms and after careful evaluation. For women, these include: lubricants, vaginal moisturizers used as the first option for vaginal dryness and used at higher frequency as needed, low dose vaginal estrogen are a second option. For those who do not respond to lubricants, lidocaine can be used for introital pain and dyspareunia, and dehydroepiandrosterone for women with vaginal/vulval atrophy.
For men; phosphodiesterase type 5 inhibitors may be beneficial for erectile dysfunction. Men who do not respond to these may consider alternative interventions such as erectile devices, medicated urethral system, or intracavernosal injections.
Behavioral therapy such as cognitive behavioral therapy, hypnosis, and medications such as Serotonin Reuptake Inhibitors (SNRI) such as venlafaxine are other options for treating sexual dysfunction.4

Conclusion
-
- Sexuality is an essential aspect of the quality of life in cancer patients. It encompasses sexual health, intimacy, reproductive health, and gender identity.
- Cancer diagnosis and treatments affect sexual function and sexuality.
- It is normal for patients to feel uncomfortable bringing up sexual health concerns to their health care providers; however, patients should understand that these concerns are valid and are a significant aspect of their quality of life.
- Quality of life is a general sense of well-being and addresses multiple dimensions of life such as physical, psychological, social, and spiritual well-being.
- Both patients and health care providers should be advocates for the patient’s best care and quality of life. This can be done through open communication on every aspect of life that the patient may not be perform optimally.
- Communication between the patient, provider, and partner (if the patient so wishes) remains the cornerstone for optimal management of sex and reproductive health concerns.
- Evidence-based interventions exist that can help address and alleviate these concerns.
- Patients should feel free to address any sexual concerns with their health care providers during cancer management. Partners are welcome into these discussions if the patient wishes.
- Numerous resources and support are available throughout cancer care to alleviate sexuality concerns. Clinicians can offer appropriate sexual counseling and treatment as necessary to improve patient’s quality of life.25

Questions to Ask About Sexuality and Lung Cancer
References
- Sexual and Reproductive Health and Research (SRH), including the Human Reproduction Programme (HRP). https://www.who.int/teams/sexual-and-reproductive-health-and-research/key-areas-of-work/sexual-health/defining-sexual-health
- Albers LF, van Belzen MA, van Batenburg C, et al. Discussing sexuality in cancer care: towards personalized information for cancer patients and survivors. Support Care Cancer. 2020;28(9):4227-4233. doi:10.1007/s00520-019-05257-3
- Sexual Health | CDC. Accessed May 19, 2021. https://www.cdc.gov/sexualhealth/Default.html
- Carter J, Lacchetti C, Andersen BL, et al. Interventions to address sexual problems in people with cancer: American society of clinical oncology clinical practice guideline adaptation of cancer care. Ontario guideline. J Clin Oncol. 2018;36(5):492-511. doi:10.1200/JCO.2017.75.8995
- Shell JA, Carolan M, Zhang Y, Meneses KD. The longitudinal effects of cancer treatment on sexuality in individuals with lung cancer. Oncol Nurs Forum. 2008;35(1):73-79. doi:10.1188/08.ONF.73-79
- Sarna L, Brown JK, Cooley ME, et al. Quality of life and meaning of illness of women with lung cancer. Oncol Nurs Forum. 2005;32(1). doi:10.1188/05.onf.e9-e19
- Williams, RN, MSNc, PHN AC, Reckamp, MD K, reeman, MSN, RN, ANP-BC, CHPN B, Sidhu, MSW, LCSW R, Grant, RN, DNSc, FAAN M. Sexuality, Lung Cancer, and the Older Adult: An Unlikely Trio? J Adv Pract Oncol. 2013;4(5):331. doi:10.6004/jadpro.2013.4.5.5
- Experts Call for More Awareness of Sexual Dysfunction in Lung Cancer Patients – The ASCO Post. Accessed May 17, 2021. https://ascopost.com/News/15070
- Reese JB, Shelby RA, Abernethy AP. Sexual concerns in lung cancer patients: An examination of predictors and moderating effects of age and gender. Support Care Cancer. 2011;19(1):161-165. doi:10.1007/s00520-010-1000-0
- Jennifer RB, Shelby RA, Abernethy Pickar Amy. Sexual concerns in lung cancer patients: an examination of predictors and m…: EBSCOhost. Supportive Care in Cancer. doi:10.1007/s00520-010-1000-0
- Lindau ST, Surawska H, Paice J, Baron SR. Communication about sexuality and intimacy in couples affected by lung cancer and their clinical-care providers. 2011;20(2):179-185. doi:10.1002/pon.1787
- Southard NZ, Keller J. The importance of assessing sexuality: A patient perspective. Clin J Oncol Nurs. 2009;13(2):213-217. doi:10.1188/09.CJON.213-217
- Bober SL, Sanchez Varela V. Sexuality in adult cancer survivors: Challenges and intervention. J Clin Oncol. 2012;30(30):3712-3719. doi:10.1200/JCO.2012.41.7915
- Flynn KE, Reese JB, Jeffery DD, et al. Patient experiences with communication about sex during and after treatment for cancer. 2012;21(6):594-601. doi:10.1002/pon.1947I
- Intimacy – APA Dictionary of Psychology. https://dictionary.apa.org/intimacy
- Sexual Intimacy During Cancer Treatment | CTCA. https://www.cancercenter.com/community/for-caregivers/intimacy-during-cancer
- Lee SJ, Schover LR, Partridge AH, et al. American Society of Clinical Oncology recommendations on fertility preservation in cancer patients. J Clin Oncol. 2006;24(18):2917-2931. doi:10.1200/JCO.2006.06.5888
- Ntekim A. Sexual Dysfunction Among Cancer Survivors. In: Sexual Dysfunctions – Special Issues. InTech; 2011. doi:10.5772/26008
- Zabora J, BrintzenhofeSzoc K, Curbow B, Hooker C, Piantadosi S. The prevalence of psychological distress by cancer site – PubMed. 2001;10(1):19-28. Accessed May 26, 2021. https://pubmed.ncbi.nlm.nih.gov/11180574/
- Lu Y, Fan S, Cui J, et al. The decline in sexual function, psychological disorders (anxiety and depression) and life satisfaction in older men: A cross-sectional study in a hospital-based population. 2020;52(5):e13559. doi:10.1111/and.13559
- Huang X, Zhang TZ, Li GH, Liu L, Xu GQ. Prevalence and correlation of anxiety and depression on the prognosis of postoperative non-small-cell lung cancer patients in North China. Medicine (Baltimore). 2020;99(11):e19087. doi:10.1097/MD.0000000000019087
- Wong ML, Paul SM, Cooper BA, et al. Predictors of the multidimensional symptom experience of lung cancer patients receiving chemotherapy. Support Care Cancer. 2017;25(6):1931-1939. doi:10.1007/s00520-017-3593-z
- Duma N. How to Maintain Your Sexual Health During and After Lung Cancer | Cancer.Net. https://www.cancer.net/blog/2020-11/how-maintain-your-sexual-health-during-and-after-lung-cancer
- Hordern AJ, Currow DC. A patient-centred approach to sexuality in the face of life-limiting illness. Med J Aust. 2003;179(6 SUPPL.):S8-S11. doi:10.5694/j.1326-5377.2003.tb05567.x
- Bolat MS, Celik B, Celik HK, Akdeniz E. The impact of thoracotomy on psychological and sexual function in men with lung cancer. Rev Int Androl. 2019;17(3):94-100. doi:10.1016/j.androl.2018.05.002